How does a TCR T-cell therapy work?
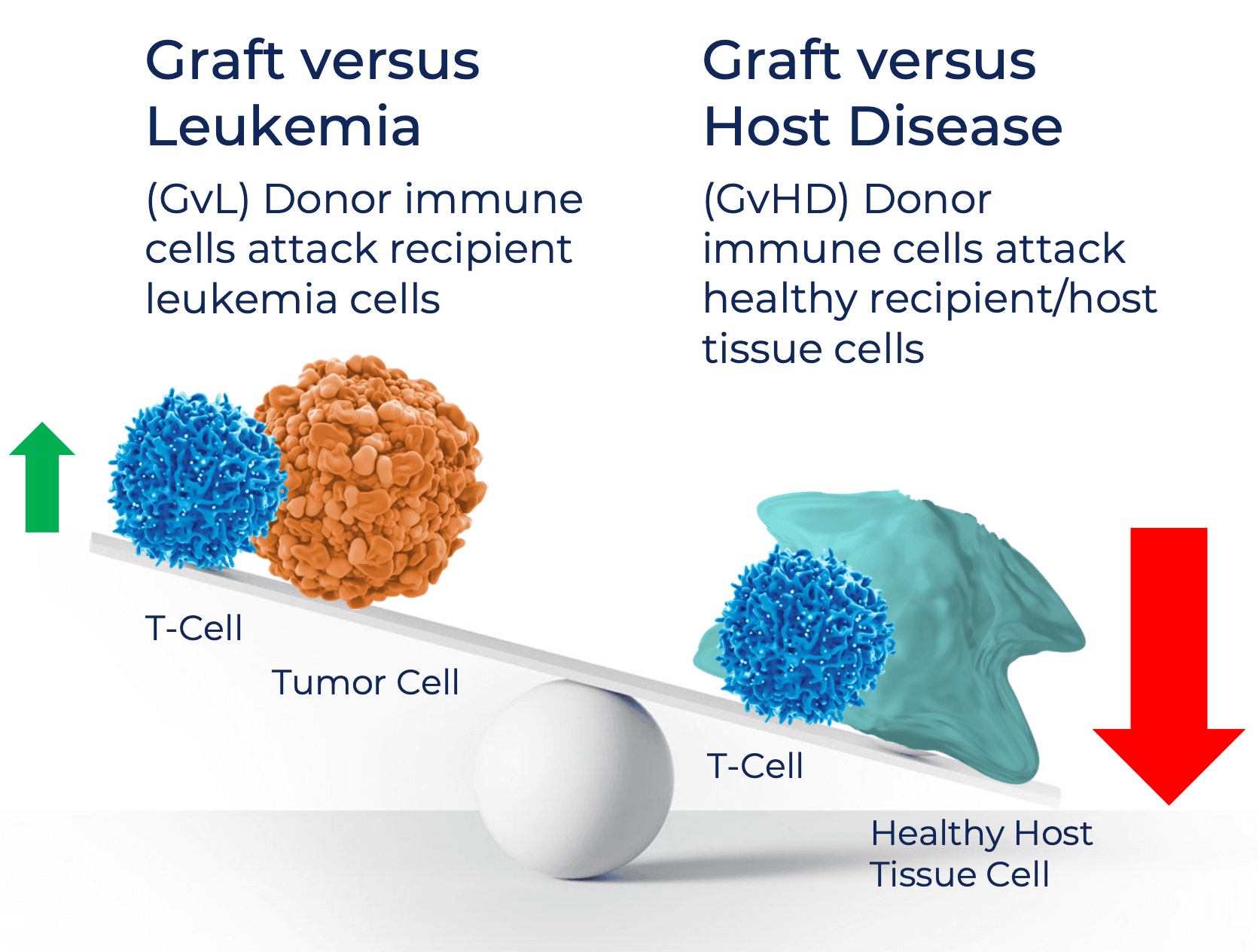
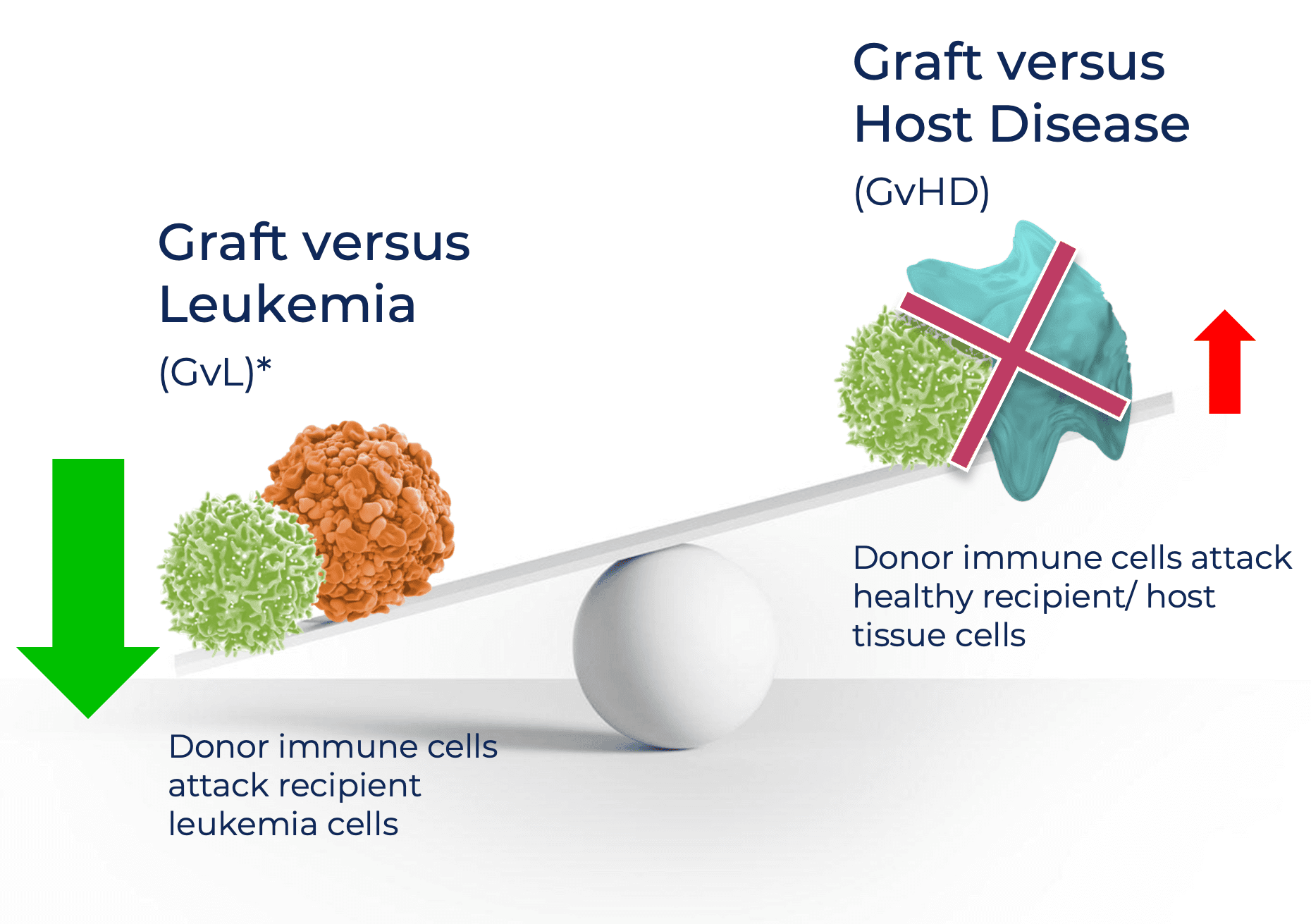
How does the blood-restricted antigen, HA-1, play a role in fighting cancer?

What about the patient’s non-cancerous blood cells getting destroyed by this TCR T-cell therapy?
What is an allogeneic stem cell transplant?